

[This article was published in the June 2015 issue of The Nugget of the Nevada County Republican Women Federated, and is reprinted here with permission. Its author is the Legislative Chair and 2nd VP of that organization.]
Jo Ann Rebane
Medicaid today has been described as a costly medical insurance financing scheme jointly funded by federal and state government general funds that delivers poor quality care to “qualifying” low income people.
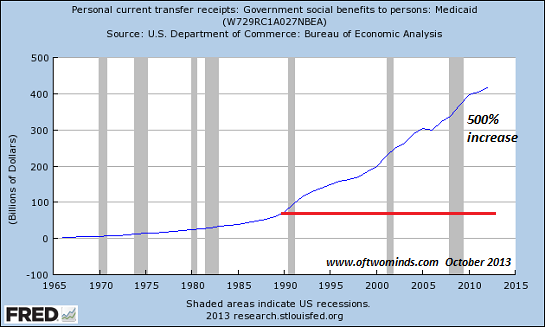
A little background: In 1965 a Democratic Congress created the Medicare parts A and B and Medicaid programs in response to President Lyndon Johnson’s “War on Poverty”. Unlike Medicare, Medicaid does not have any independent revenue source or trust fund, enjoying open ended access to the federal government’s general fund with no defined limits. Over the years Medicaid eligibility standards have loosened and enrollment numbers have increased. And philosophically Medicaid has been viewed by some as a first step in government supplied universal healthcare that establishes a “right” to healthcare.
Medicaid is a means-tested program which in 2013 paid for medical and long-term care for some 72 million low income individuals, children, disabled, and elderly – one fifth of the US population. All states have elected to participate in Medicaid, have established and administer their own programs, agree to pay for services provided to enrollees and thereby have a legal right to federal matching payments for those medical services with no upper limit. Federal reimbursement rates to the states are a percentage tied to state per capita income. California enjoys a 50% reimbursement rate and in 2011 received more than 12% of all federal Medicaid spending. With enactment of Obamacare, states are encouraged to expand Medicaid to all US citizens and legal residents with income up to 138% of the poverty line, with the federal government covering all expansion costs only through 2016.
State programs must offer a minimum set of medical benefits. But states are free to impose their own income thresholds and enlarge the scope of services beyond those mandated, as well as determine whether to require premium payments, copayments, and deductibles in response to their own unique economic and political pressures. The impact on federal spending, because of the matching formula, is directly affected by the design of the several states programs. The matching regimen provides little incentive for states to reign in program costs. The Association of State Budget Officers estimated that Medicaid was 23.9% of all state government spending in 2012, more than spending on elementary and secondary education which averaged 19.8%.
California’s Medicaid program, Medi-Cal, covered about 11 million people as of mid 2014, which is about 30% of all Californians. While Medi-Cal provides vital benefits to low-income residents, the program’s size strains state resources. Medi-Cal expenses exceeded $50 Billion, half of which was reimbursed by the federal government in fiscal 2012 and in 2014-15 will require $29 Billion (the unreimbursed portion) or 27% of the state’s general fund.
Closer to home in Nevada County, as of last month 19,819 residents or 20% of the population is enrolled in Medi-Cal, up from 11% in 2013 due to expanded access from Obamacare. The 38 “eligibility” employees from the Health and Human Services agency, among their other tasks act as state agents to determine the eligibility status of potential enrollees. The county is reimbursed by the state for that service. Locally, 3 Federally Qualified Health Centers like Western Sierra Medical Clinic and Sierra Family Medical Clinic accept patients covered by Medi-Cal as do our two hospitals (Truckee and SNMH), facilities which have not expanded to handle the increased patient load. (I appreciate the assistance of Alison Lehman and Martin Polk of the County Executive’s Office providing this and other information.)
Nationwide Medicaid enrollees complain of difficulties getting timely appointments from the few doctors who still accept the very low state payment schedules. An American College of Emergency Physicians recent survey notes since inception of Obamacare and the increased numbers of people covered by Medicaid, more patients are ending up in the ER where crowding has been linked to longer wait times and poorer outcomes. Moreover, without an economic turnaround, the ranks of the poor will not shrink. Actuaries from the Centers for Medicare and Medicaid Services (CMS) predicted Medicaid expansion would “… greatly increase demand for health services, and soaring demand always increases prices and costs.” Whether from rising healthcare costs, changing demographics, increased eligibility, service expansions, and/or waste, Medicaid continues to become a larger share of states’ and the federal budgets. And therefore is an unsustainable solution to provide healthcare services, let alone quality healthcare.
There’s no argument that the poor need healthcare, and until we find a better way, government, as a last resort, will provide it. But, in my view, the current set-up needs to be revamped. As with most state/federal programs, politicians, in order to secure votes have promised more services for more people, year after year. Added program services strain budgets. In order to pay for the expanded programs, other programs must be cut, taxes increased and/or debt levels raised. Without reform, Medicaid is a system which harms all of us – federal and state taxpayers, healthcare providers, and the poor. We all lose.

{kind=link}
{kind=link}
Leave a comment